
The purpose of these transitional living facilities is to provide the unsheltered homeless population with a place to receive medical care, job training, and to undergo rehabilitation in order to rejoin society. Complexes should function as small towns, complete with medical facilities, gyms, living facilities, recreational areas, and more, all of which will assist in the reorientation of individuals who are not undergoing significant mental health, criminal, or substance abuse problems. Frequent monitoring via technological means such as cameras and other sensors will allow for a safer living environment and a more productive program overall.
It is best to begin the design of these complexes with standard transitional living facilities as they do not require extensive parallel services, as would be the case with mental health complexes and substance abuse facilities. From this blueprint, adaptations can be made to expand the size of the complexes themselves, and also to add or expand parallel services in instances where more support is needed at any given facility, offering flexibility through a centralized system. Large complexes allow for greater pools of resources than could be achieved with significantly smaller complexes, resulting in greater efficiency in key areas of the rehabilitation process, such as medical care, therapy, job training, and related services.
Beginning at the smallest level for the sake of comprehension, the individual room is an 8 x 10’ space complete with a twin sized bed, a personal wardrobe, and a small desk and chair. The room itself will be accessed through electronic locking systems that will be activated by the worn monitors of the resident. These monitors would most likely take the form of ankle monitors, but their specific design remains outside of the scope of this specific article. Electronic locking systems allow for remote access, allowing both the resident and staff to access the room as needed while still offering privacy that can only come with locked living quarters.
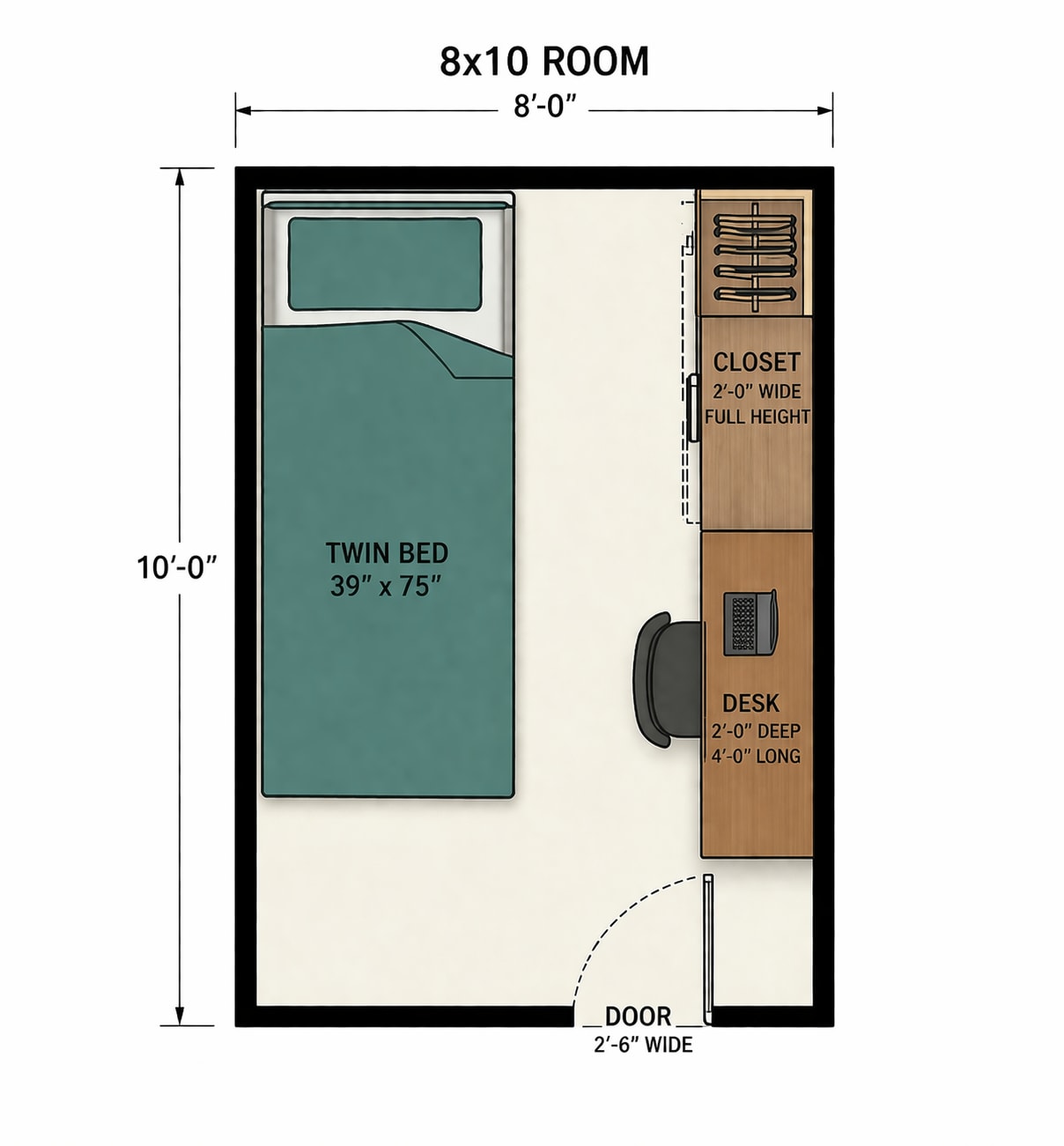
As can be seen in the diagram of the room, only one inhabitant is permitted, and this can be enforced through hallway cameras and resident tracking and monitoring. The individual rooms reduce the likelihood of theft, while also increasing safety and reducing the likelihood of interpersonal conflict between residents. This effectively offers a stable living environment for those who manage to obey the rules of the facility, allowing for proper rehabilitation.
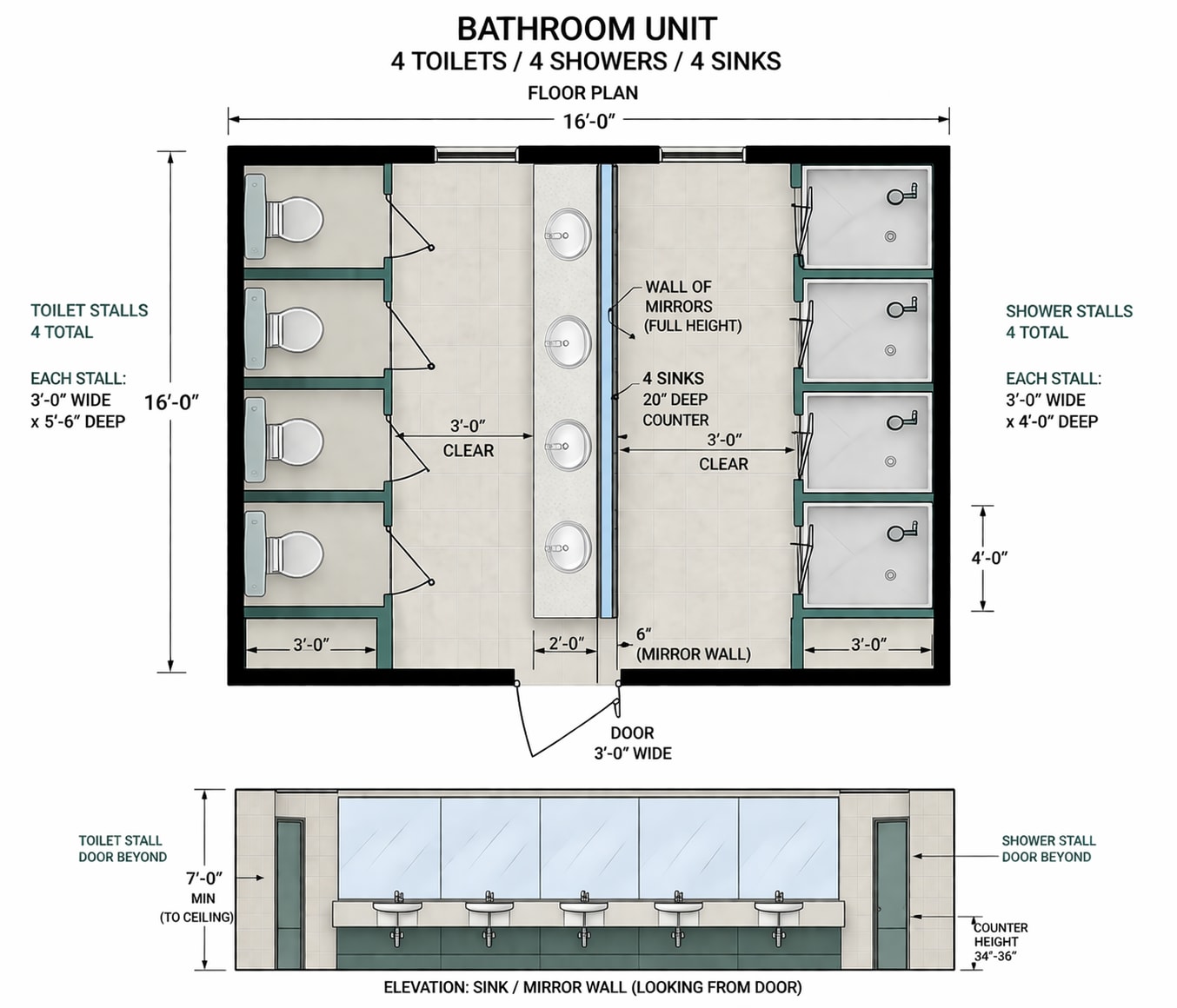
Bathrooms will be shared amongst a unit consisting of 24 individuals, consisting of four sinks, four bathroom stalls, and four showers. The ratio of individuals to shower, wash basin, and toilet exceeds that of OSHA standards under this plan, providing for a generous and comfortable living environment for the resident. The grouping of 24 individual bedrooms and a single bathroom represents a unit, of which each floor hallway will have five. Every residential building of the complex will have three total floors with two main hallways per floor, housing 720 people per building. In total, a complex that is expected to house 10,000 individuals will require 14 residential buildings in order to achieve that objective.
A standard complex of 14 residences capable of maintaining a total of 10,080 occupants should be accompanied by a medical facility, administrative building, charity shops, and other stores, a cafeteria, career training facilities, a gym, and recreational areas, all interconnected by roads and walking paths. The necessary parking lots outside of the residences will likely not require as many spots as will the administrative and medical buildings, due to the likelihood of the homeless occupants not having vehicles at the time of their arrival.

The medical facility itself is crucial to the proper operation of the complex, as unsheltered homeless people are at significantly higher risk of medical conditions, and many will need treatment for various illnesses resulting from their lifestyle. While this complex is not designed for the treatment of mental health patients, nor seriously addicted individuals, therapists and drug abuse counselors should nonetheless have an active role in the medical treatment of the residents as needed. The purpose of this medical facility is not to provide extensive treatment, such as major surgery, but rather to treat common injuries and illnesses, and to serve as a point of referral for the residents to other providers as needed. This ensures that the population is as healthy as possible and better able to integrate with fewer resources after their rehabilitation has concluded.
The administrative building functions as a hub for the entire campus, where new residents will be given orientation, and meet with career counselors and other services. Complex police and security staff will also maintain a presence on campus, with their headquarters being located inside of the administrative building itself.
Charity shops, thrift stores, and other low-price stores that sell or donate necessities should be attached to the administrative building and positioned along the main corridor, allowing for easy access by residents.
Career training facilities offer residents the ability to learn vocational skills and other job skills that could secure their future once they transition out of the facility. These programs may include, but are not limited to, construction trades, mechanical trades, maintenance and facilities management, logistics and warehousing, food service, administrative support roles, and entry-level security training.
An on-campus gym allows for residents to regain or maintain their physical health through exercise, along with recreational fields and other paths for walking or cycling. Access to the gym and other facilities will follow similar patterns of traffic to that of the cafeteria, allowing all to access during preplanned slots depending on population and occupancy limitations.
The scale of the population, as well as the rates of criminal conduct, substance abuse, and mental health disorders within the general homeless population creates heightened security concerns for the complex. Due to the size of the resident population and the elevated baseline risk, a small police department composed of fully qualified law enforcement officers will be necessary to maintain order. In addition to the police force itself, technological systems, such as cameras and individual monitors, offer a force multiplier for the officers in managing the population. Residents who meet certain requirements involving conduct, length of stay, and training can also take on a security role, patrolling their floors and the wider campus under the direct supervision of dedicated officers. This sort of role could offer a career pipeline into unarmed security positions and allow for the role to be carried out on site without the need for expensive private contractors.
The objective of this program is not to control and violate the individual, but rather to offer them a safe and healthy environment to regain stability and facilitate reentry into society. It is for this reason that security cameras are needed in all public areas in order to monitor the many floors of all the buildings as well as the outdoor campus. Close monitoring can reduce criminal behavior and quickly address other emergencies that may arise such as fire or medical incidents. These cameras should be monitored as CCTV by appropriate staff, as well as artificial intelligence systems that watch for and flag suspicious conduct, including violations of the rules, such as multiple residents in a single bedroom or unapproved access to other resident halls. One camera, properly positioned and capable of seeing the unit’s entry into the hallway as well as all 24 bedrooms and the entrance to the bathroom is needed for every unit. For this reason, 10 cameras should be adequate if properly located per floor, meaning 30 internal cameras per building. Additionally, 12 total exterior cameras, one at every entrance, and two positioned on the roof of every building will offer a satisfactory field of coverage inside and outside of the residency structures. Security can be further supported through the proper sorting of demographics upon admission, a topic for future analysis.

Automated security systems, such as patrol drones, both manned and unmanned, which may take the shape of nearly consumer off-the-shelf models, should also be considered, as well as wheeled automated patrol vehicles. These measures significantly increase the footprint of security and assist in ensuring the safety of the residents and the continued well-being of the facilities.
Ankle monitors that can be remotely accessed and viewed can provide the individual with electronic access to their rooms and other facilities without the need for additional keys or passcodes, while also enabling automated location tracking to ensure they are not in restricted areas, have not left the premises, or to locate them if the need were to arise. This combination of protocols and technology allows for maximum privacy in their individual bedrooms while also supplying the needed order and infrastructure that allows for it.
Drug testing and related measures demonstrate a position at the intersection of administrative policy and security systems. Some individuals who are mentally ill, addicted to substances, or have criminal proclivities will inevitably slip through any mass-scale filtering measures, necessitating structured security posture and protocol to handle such cases. Individuals who are found to have violated the rules of the facility, consumed illicit drugs, or violated the law in a minor way will be referred to review and judgment by a panel of judges and experts, who will determine an appropriate response, whether it be labor outside of the complex, extra labor within the complex, or referral to criminal courts. The development of these criminal justice and judicial standards and protocols will need to be elaborated at a later date, as it exceeds the scope of this examination. In this way, both incentives and consequences are clearly defined and strictly enforced, allowing the individual to take charge of their lives in a comfortable and safe environment, while also maintaining clear boundaries of conduct and progression within the program.
Individual bedrooms must be regularly inspected and this can be accomplished through dedicated resident roles who work directly with administration. One of the most efficient and effective ways to carry out these room inspections is through a resident representative who will be granted access to floors and bedrooms for a set interval, requiring an active body cam and the carrying of a camera. These measures ensure that they are not overlooking misconduct, as there will be supervision and they will be assisting in the inspection of rooms on other floors. The resident representative will enter the room and visually inspect it to ensure its cleanliness and that it is up to standards, and then will activate a 360 camera which will scan and record the state of the room. AI can additionally be used at this stage to flag obvious problems, increasing the likelihood that damage to rooms will be caught early on and that standards can be upheld without cameras being constantly in the individual room. Maintenance will be similarly carried out by both paid staff and resident laborers who will work as assistants in teams to complete safety and cleanliness checks.
Administration is responsible for the residents from intake to discharge. An orientation class should be offered where the standards and rules are clearly established by administrative staff. An explanation of request forms and the supply of necessary living essentials should also be conducted in this early stage. Shortly after, new intakes should meet with career counselors, other advisors, psychiatrists, and medical doctors. Through this process, the individual can be fully cleared for work and decide on a path that meets their desires and for which they qualify according to their tested aptitudes and work history. Work roles and vocational/educational courses will then be assigned, and the individual will be expected to maintain their schedule accordingly, as well as all standards explained to them.

Under the system, an average resident might be expected to work on-site or off-site for 5-6 hours per day and to attend 2 to 3 hours of vocational training per day. This allows for ample time for recovery, medical visits, therapy sessions, and additional services, to which many previously homeless residents will require access.
Due to a necessary restriction on cooking appliances, the cafeteria will need to serve all of the residents. This is no simple feat and cannot be completed with one cafeteria alone and without periods of restricted access, requiring a central kitchen to operate in the cafeteria or other preparatory elements operating on campus outside of the cafeteria itself. In order to serve all residents, a weekly rotation is needed, where a fraction of the total population will be permitted to dine at the cafeteria, and the rest will have food delivered to their buildings and distributed by resident workers. This ensures that all residents receive hot meals and have a place to eat, even if it is in their unit’s common area.
Scheduled items such as dining rotations can be updated to a central system that will notify appropriate residents on their issued smartphones. These devices will be limited and tracked but will allow for residents to keep track of scheduled shifts, receive emergency notifications, request medical attention, and be contacted directly.
Similar to the cafeteria, recreational fields and the gym will be open according to a rotation by resident floor, which will be visible on their provided device. The ultimate objective of this transitional complex is to stabilize the individual and to set them up for success and reintegration. This may come about through multiple pipelines:
-
The individual is taught skills or otherwise connected with private employers and transitioned back into the community with gainful employment.
-
The individual and the state are unable to find private placement, but are utilized in state programs, such as those that do disaster cleanup, infrastructure management, construction, military, service, etc.
-
The individual secures a position at a place of higher learning and finds the financial means to support themselves through loans or scholarship.
Those who prove themselves incapable of reintegration will need to be referred to an appropriate panel of experts who will determine the course of their transition, wherever that may be. A set limit on residency should not be established, although soft limits should be put in place to ensure that individuals have not stagnated in such a comfortable environment, choosing to remain as long as possible instead of rehabilitating. These limits should be set by their panel of providers, including social workers and career advisors, in order to ensure that each person is given the individualized focus needed to best assist them.
Pricing
With double-loaded hallways, complete with 6’ corridors, amounting to an estimated length of 960’ per hallway, and a total square footage of 74,880 per three-story building, 14 identical residential buildings amount to a total of 1,048,320 sq ft. Current (2026) estimates of commercial building costs are commonly cited between $220–$280 per square foot, indicating that each building will likely cost between $16.47-$20.97M, for a total range of $230.6-$293.6M for all residential structures, assuming commercial construction estimates. Construction costs thus amount to around $22,900 per room for the residential facilities. The other primary facilities will be listed accordingly.
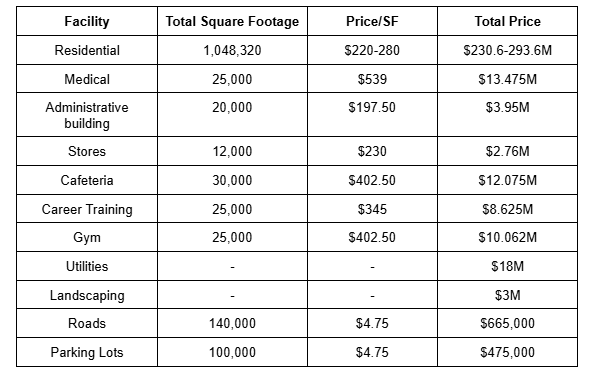
The total after all of these facilities are constructed through commercial construction methods amounts to $329.9M, and after including “soft costs” such as engineers and architects, the total project amounts to around $440M. Of this $440M total, around $155-$200M would be related to labor costs. It is for this reason that it is proposed to utilize a fraction of the 80-90,000 U.S. military personnel across active duty, reserve, and National Guard engineering units. Additionally, there are approximately 300,000-500,000 inmates within the United States in low/minimum security prisons, many of whom are serving relatively minor sentences. Supervised work programs for the most well-behaved inmates could further serve their rehabilitation and reintegration process, as well as allow for earlier release based on demonstrated conduct and participation.
A primary workforce of 30,000 U.S. troops and 20,000 inmates (along with their supervising structure) could significantly reduce labor-related costs, potentially by up to $150M per complex. It should be noted that it is not suggested that a workforce of 50,000 people is required for a single complex, but rather that 4,000-6,000 workers be actively deployed at any one location at a time to allow for efficient and continuous construction across multiple phases:
Phase 1: Site prep and utilities (1-3 months)
Phase 2: Foundations and utility trunks (2-4 months, overlapping with site prep)
Phase 3: Residential structures (4-8 months, heavily parallelized across all 14 buildings)
Phase 4: Support buildings and interiors (3-6 months, overlapping with structural work)
Phase 5: Final paving, testing (1-3 months)
Through a workforce of this size and structure, along with their proper management, a transitional complex as described could cost as little as $290M, significantly reducing the private contractor’s estimate of $440M. These costs could be further reduced through a nationalized approach to the purchasing of the raw materials themselves, which may take many forms. Depending on a range of logistical and environmental factors, a complex of this scale could be completed in as little as six months under highly optimized conditions, or more realistically within 12–18 months.
Jake LeoneRead More








 T1
T1



