
Homelessness is often discussed, but very rarely are comprehensive, far-reaching strategies presented, with most suggestions and implementation occurring on local levels. On the surface, homelessness seems to be easily solved: simply build houses. Unfortunately, the problem is far too multifaceted to have such a simple solution. Houses and apartments can be built for the homeless, but without appropriately addressing the cause of the individual’s homelessness, such as substance dependency or chronic mental health issues, there is a non-negligible likelihood that the lifestyles of the newly housed will continue functioning in a similarly dysfunctional manner. This essay contends that homelessness in modern America can be solved through the development of specific systems, new legal standards, and updated enforcement methods, and it will provide a brief overview of such to prepare the intellectual foundation for subsequent essays.
The first step to properly addressing the problem at hand will be to analyze the data surrounding homelessness, including racial, age, and gender demographics. Additionally, adjacent systems such as those that deal with mental health, medical care, and incarceration will need to be evaluated to a certain extent in order to best understand their interaction with the modern homeless problem. After the problem is clearly outlined, practical solutions can be developed according to the data.
The US Department of Housing and Urban Development’s 2024 annual homelessness assessment report to Congress asserted that 2024 had been the highest recorded year yet, with 771,480 homeless being recorded across the country.1
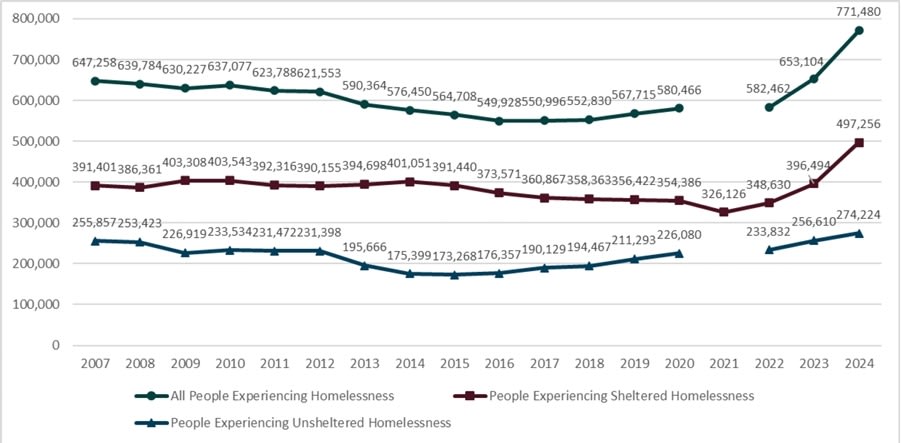
Data in the graph from the US Department of Housing shows a relatively stable homeless population until around 2022, where a sharp increase could be seen leading to the figures taken in 2024. While the specifics regarding currently sheltered and unsheltered individuals do demonstrate some level of functionality within the context of the American homeless crisis, this functionality remains insufficient relative to the scale of the problem, and due to its inefficiency and proven inability to function at the level which is demanded of it, it should not be blindly inherited. Blind inclusion of these shelters and systems may cause even more drag on an updated, purpose-built national system than assistance.
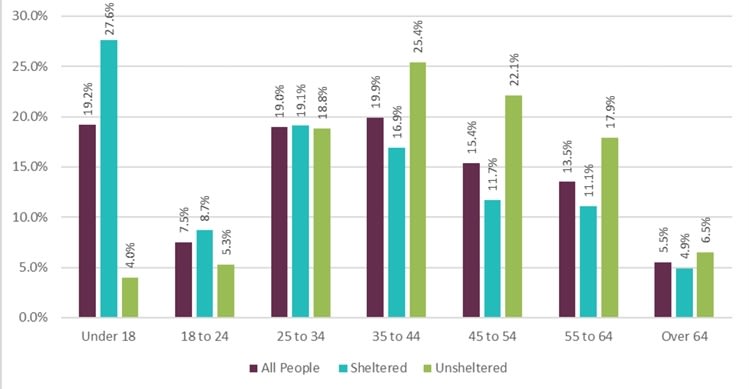
HUD’s demographic data offers a crucial insight into the origins and continuation of homelessness in America. The age range from 35 to 44 has the highest representation of homelessness, closely followed by the under 18 demographic and the 25 to 34 demographic. A significant dip from 19.2% to 7.5% can be seen from the juvenile age demographic to the 18 to 24 age range, indicating a possible correlation with the age of adulthood and the transition point to self-supported living. Some research suggests that this drop represents mostly a reduction in the services used to track the individual’s homeless status, rather than a true reduction in homelessness, demonstrating a possible underrepresentation in official counts.
Additionally, it appears that after the spike from 35 to 44, the population considerably drops with each subsequent data set. This decline is likely explained by a combination of mortality rates, institutionalization, and incarceration. Due to substance abuse, increased exposure to violence, untreated medical conditions, and exposure to the elements, chronic homelessness is closely tied to a reduction in life expectancy, explaining the tail end of this distribution.
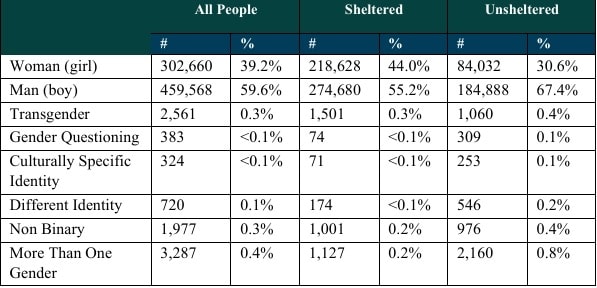
When gender demographics are taken into account, men represent about 60% of the homeless population, while women represent about 40%. Furthermore, over 72% of homeless women were sheltered in 2024, whereas 59% of men were sheltered in the same year. This demonstrates a disproportionate access to shelter-based services among women within the current system, and indicates that the majority of unsheltered homeless who would be apprehended under this policy would be men, which is an important insight for facility planning.2
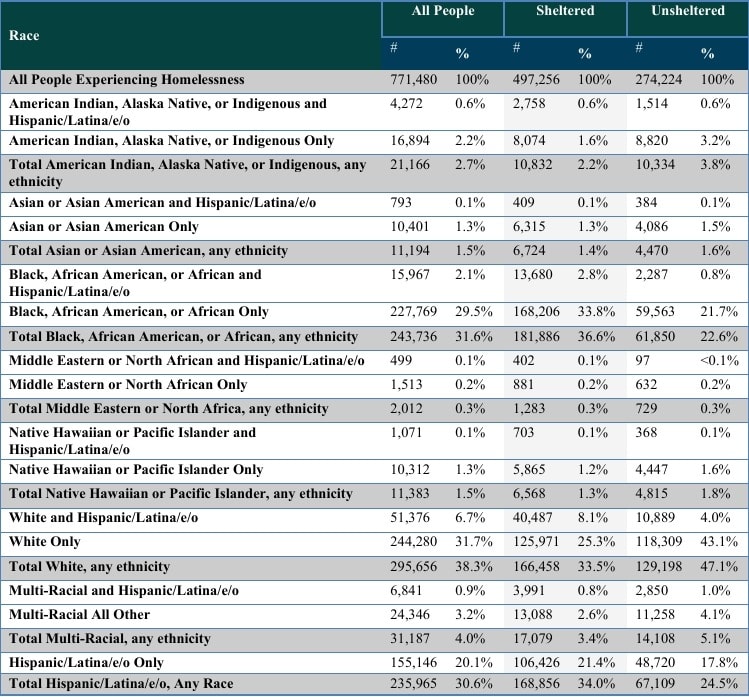
Finally, when looking towards the racial demographics of homelessness, it is found that only 244,280 of the total 771,480 homeless people are white, representing only 31% of the total homeless population. While each one of these data sets are interesting on their own and do warrant further investigation, for the purposes of this analysis, they will simply be taken at face value.
Some studies found that 54% of homeless individuals who were receiving services had been incarcerated in the past, and that of those who were incarcerated the average was nineteen, whereas the general population’s incarcerated demographic had four.3 Clearly, there is a massive criminal and mental health element to homelessness that must be recognized, as both of these factors influence the appropriate measures that must be taken. Treating individuals who are simply mentally ill as criminals, or criminals as simply mentally ill, is equally problematic to the effective enforcement of law, maintenance of order, and the upholding of national obligation toward the well-being of the individual.
Mental illness
As previously discussed, mental illness and substance abuse are persistent problems for the vast majority of homeless individuals in America. Typically, in order to admit someone to a mental health treatment facility against their will, evidence of grave inability to care for oneself, suicidality, or homicidal intentions must be documented or attested to. If one element that could qualify the standard is the inability to care for oneself, then it can be reasonably inferred that the current system is failing to maintain these standards, as evidenced by the visible presence of individuals living in neglect across all major urban areas. Available data suggests that between 25-50% of the American homeless population is affected with serious mental health issues. This indicates a growing population of mentally ill homeless, which, when paired with a total decrease in psychiatric beds available, presents a structural incapacity within the current system. Clearly, the identification and apprehension of the mentally ill who are incapable of caring for themselves is failing at some point, possibly multiple points. Some have suggested that this fracture point could be with policing itself, and others attribute it to the reduction in mental health facilities and access to health care.
Placement
The outcomes of incorrect placement of homeless individuals are problematic to the efficiency of the operation, besides of course the ethical concerns associated with misplacement. The objective should not be to entangle homeless people into a system that perpetuates an unnecessary hurdle to the healthy rejoining of society. The concept that people should be treated according to their specific medical, psychological, and criminal circumstances is hardly controversial on its own, but becomes so when the discussion of placement is brought up. The ethical concerns relating to forced placement of homeless individuals will need to be reserved for a future essay as this work is focused on the practical applications necessary to solve American homelessness. It is for these reasons that homelessness must be approached through classification, not as a singular condition, in order to be effectively resolved.
Of the almost 800,000 homeless individuals in America, 60% are housed in temporary shelters. The initial focus of the multi-step plan proposed within this work is primarily regarding the unhoused populations, as they are not only at greater risk themselves medically due to environmental factors, but also pose a greater hindrance on the wider society in the form of crime and presence. Law must be altered to allow for greater police power in apprehending vagrants and forcefully bringing them to an appropriate destination for their unique circumstance. The specifics of these laws and the limitations, as well as the oversight and accountability relating to their implementation, will need to be examined in a subsequent essay.
In order to effectively serve both society and the well-being of the homeless population, there should be four paths from the point of apprehension.
-
Jail
-
Mental health facility
-
Rehabilitation facility
-
Transitional housing
Individuals who are contacted by law enforcement due to illegal conduct beyond vagrancy or drug use, and with no evident signs of mental illness, should be brought to jail where they can be further sorted within the criminal justice system. This essay is not suggesting that the current criminal justice system is adequately equipped, nor directed toward the same ends as would be required for success, but rather that its complete outline exceeds the scope of this essay. Nuance is also needed to respect the ethical and logical balance that must be recognized depending on the severity of the criminal conduct, so as to not reroute the criminal or particularly dangerous homeless population into treatment facilities, thereby impacting the treatment of others, and the danger to both patients and staff. One source asserts that 35 to 50% of homeless arrests are due to the legality of homelessness itself in one form or another.4
The appropriate filtering of populations will reduce the burden on the judicial system, as well as local law enforcement over time. In this way homelessness does not become decriminalized, but rather that effective measures are put in place to properly rehabilitate individuals instead of simple incarceration or treatment and release.
Sources reveal a range of results from 25–50% of the homeless population being severely mentally ill, in need of mental health treatment. This presents a major burden on mental health treatment facilities, and an operational impossibility under the current system constraints in place throughout America. The purpose of these facilities would be to triage and treat what could amount to around 75,000 to 150,000 people of the around 300,000 unsheltered homeless on the streets of America. With some of the largest mental health facilities in America currently operating only at around 1,500 beds, the extent of services required to treat 75,000 to 150,000 mentally ill individuals across the country can be fully contextualized. One mental health facility called Pilgrim State Hospital once housed almost 14,000 patients at one time during its peak years in the 1950s. While modern mental health facilities may differ significantly from those that have existed 70 years prior, it should be noted that facilities containing 10,000+ individuals are legitimately possible, as has been proven historically, with more archaic treatment techniques and less capable technology than currently at our disposal.
While the design of the facilities and day-to-day operations are best left for future research, ten mental health complexes dispersed across the country correlating to population density are suggested. Each one of these complexes should be adequately equipped in space, staff, and all other necessary resources to care for 10,000 patients per facility, specifically those who are facing homelessness. This specialization is beneficial as homeless populations have unique mental and physical health difficulties that can be best handled by dedicated treatment staff and facilities, and due to the abundance of patients in need of such treatment, the expansion of this specialization is warranted.
Some research indicates that up to 50% of the homeless population may have significant substance abuse issues, and there is undoubtedly an overlap between substance abuse and mental health statistics within homeless populations, a problem that staff working at these facilities will need to manage according to the best interest of the patient and while upholding the standardized policy that should be put in place regarding treatment. Similar to the program for the mental health treatment complexes, the development of ten nationwide rehabilitation facilities would allow for the proper placement of the drug-addicted unsheltered homeless population who are in more urgent need of rehabilitation services than mental health treatment.
Finally, there will be unsheltered homeless individuals who have not committed any crimes, are not severely mentally ill, and are not addicted to substances, and who will not benefit from a stay in jail, a mental health facility, or a rehabilitation facility. It is for this demographic that an initial fifteen transitory living complexes should be erected, similarly according to population density. More of these transitional living complexes must be initially built to manage not only those who are picked up at the start of the new standards implementation, but also to house those who have completed their treatments or incarceration so as to not further burden those systems with their malingering. Again, the specifics of these complexes and their operation are to be left to later designated research so as to not convolute the overview being presented. Due to the overlap between the statistics of mentally ill and drug-addicted homeless individuals, exact numbers regarding who would be eligible for such a transitional living facility will vary depending on the data used. Additionally, the total required beds across all the transitional complexes will also be dependent on the specific policies of such facilities, and the average length of stay. It could be estimated that initial intakes for such facilities could total 40% of the unsheltered population, amounting to 120,000, likely the largest single demographic, especially in the mid and long term when others transition out of parallel facilities.
In total, this means 35 permanent complexes positioned across the US, each capable of housing 10,000 individuals each, effectively allowing for the redirection of unsheltered populations off of the street immediately while more long-term solutions and programs geared toward the sheltered homeless population are developed. Due to the greater efficiency of properly state-managed complexes, it would be beneficial to phase out the shelters that would initially care for the population that wasn’t being immediately routed to the newly built complexes. The transition from independent facilities that operate off of community or state assistance would need to be gradual in order to not flood an already new system with additional residents. The centralization of these facilities additionally allows for more specialization in areas outside of mental and physical health, including programs such as education, employment, and life skills, etc.
Phase 1: legislation and planning
It is in the first phase that laws must be changed to allow police to apprehend unsheltered vagrants and compel either their treatment or placement. Specifics regarding regional triage locations, transportation to and from facilities, and locations of facilities, as well as their necessary infrastructure, will need to be properly laid out before the beginning of this phase.
Phase 2: infrastructure development
Enforcement of the previous legislation will not be enacted until after phase 2 is complete so as to ensure that facilities are capable of managing the unsheltered population. Through incarcerated labor, military involvement, and any additional contractors needed, facilities can be constructed in relatively short periods of time.
Phase 3: enforcement on unsheltered homeless
Phase 3 begins the enforcement period, where legislation comes into effect and unsheltered homeless individuals are diverted away from cities to triage locations and then to their respective treatment facility or transitional housing location.
Phase 4: development of additional infrastructure to house the sheltered
It is in phase four where enforcement continues, adjustments to facilities and their operations are ongoing so as to improve efficiency and effectiveness of treatment, and where private shelters that are publicly funded become centralized in the name of efficiency and effectiveness.
Subsequent essays will expand on the specific aspects of this overview, demonstrating the feasibility of the plan through the resources and institutional capacities available in the modern American context.
References
-
U.S. Department of Housing and Urban Development. The 2024 Annual Homelessness Assessment Report (AHAR) to Congress: Part 1: Point-in-Time Estimates of Homelessness. December 2024.
-
Ibid.
-
Metraux, Stephen, Caterina G. Roman, and Richard S. Cho. “Incarceration and Homelessness.” In National Symposium on Homelessness Research, Washington, DC: U.S. Department of Housing and Urban Development, 2007.
-
Zeng, Zhen. Jail Inmates in 2022-Statistical Tables. Washington, DC: Bureau of Justice Statistics, December 2023.
Jake LeoneRead More








 T1
T1



